Best Antibiotic for a UTI in Canada? Options Explained
There is no single best UTI antibiotic for everyone. A clinician chooses treatment based on your symptoms, pregnancy status, allergies, kidney function, past cultures, recent antibiotic use, and local resistance. This guide explains commonly considered options for uncomplicated bladder infections and the warning signs that require testing or urgent in-person care.
Book Your Appointment Now
The best antibiotic for a UTI depends on whether the infection is uncomplicated, your allergies, kidney function, pregnancy status, recent antibiotics, past urine cultures, and local resistance. Nitrofurantoin, fosfomycin, or trimethoprim-sulfamethoxazole may be considered for suitable uncomplicated bladder infections, but a clinician must choose the treatment and dose.
- Antibiotic selection and duration depend on the diagnosis, patient factors, local guidance, and culture results when testing is needed.
- A urine culture is more likely to be needed for pregnancy, recurrent infection, treatment failure, male patients, or complicated symptoms.
- Symptoms often begin to improve within 48 hours of effective treatment; worsening symptoms or no improvement require reassessment.
- Recurrent UTI defined as 2 or more infections in 6 months or 3 or more in 12 months
Clinical content is reviewed for accuracy and scope. TelePlus Care appointments go ahead only when a doctor agrees it is the right call, after a real assessment, and the doctor will explain the next step if virtual care is not the right fit.
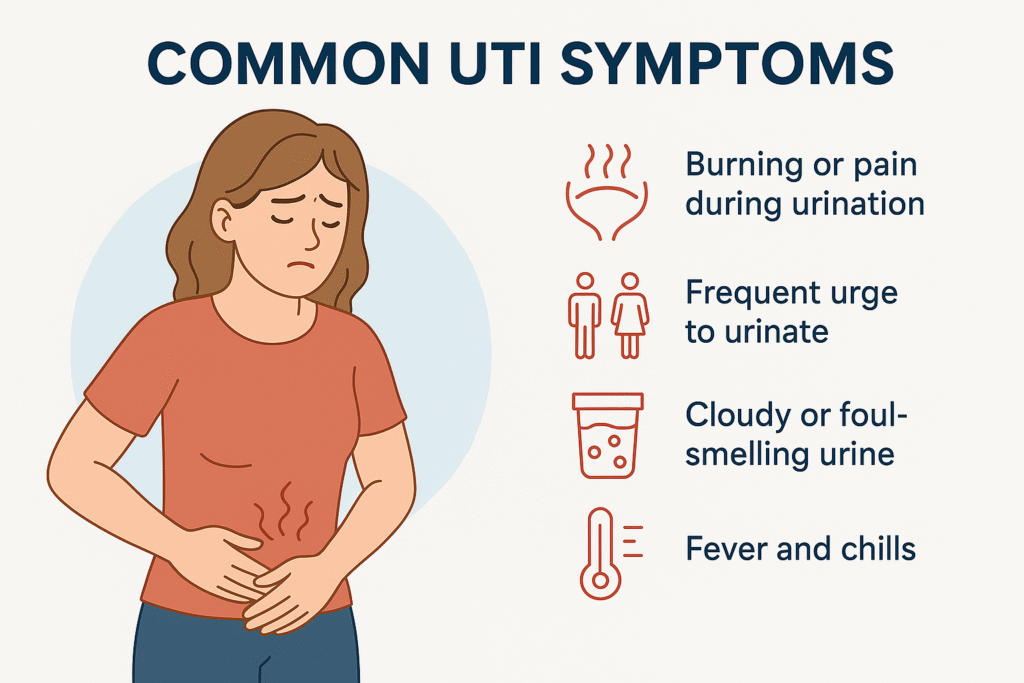
What Is a UTI and Why Antibiotics Are the Standard Treatment
A urinary tract infection (UTI) happens when bacteria — most commonly Escherichia coli from the bowel — climb the urethra and colonize the bladder. The bladder lining becomes inflamed, producing the burning, urgency, frequency, and pelvic pressure most patients recognize within hours of onset. Because UTIs are caused by bacteria, they require antibiotics to clear; hydration, cranberry products, and over-the-counter analgesics like phenazopyridine relieve symptoms but do not eradicate the infection. Untreated lower-tract UTIs can ascend the ureters and seed the kidneys, producing pyelonephritis — a more serious infection associated with fever, flank pain, nausea, and the risk of bacteremia. For this reason Canadian guidance from AMMI Canada (the Association of Medical Microbiology and Infectious Disease Canada) and the Infectious Diseases Society of America recommends prompt empiric antibiotic therapy for symptomatic UTIs, with antibiotic choice guided by patient factors and local resistance patterns. A doctor assessment is required — antibiotics in Canada are prescription-only and self-treating with leftover or borrowed medication risks resistance and incomplete cure.
First-Line UTI Antibiotics in Canada: The Top Three
AMMI Canada and IDSA guidelines name three first-line agents for uncomplicated cystitis (bladder infection) in non-pregnant women. Each has a distinct dosing schedule, side-effect profile, and best-fit patient. Your doctor will recommend one based on your allergies, kidney function, prior antibiotic exposure, and whether you are pregnant or breastfeeding.
- Nitrofurantoin (Macrobid, Macrodantin) — 100mg by mouth twice daily for 5 days. Highly active against E. coli with very low Canadian resistance. Concentrates in the bladder, so it is ideal for cystitis but not for kidney infection. Avoid if creatinine clearance is below approximately 30 mL/min.
- Fosfomycin (Monurol) — 3g sachet dissolved in water as a single dose. Useful when adherence is a concern or when a patient prefers one-and-done dosing. Effective against most multi-drug-resistant E. coli strains. Take on an empty stomach.
- Trimethoprim-sulfamethoxazole (Bactrim, Septra) DS — one double-strength tablet twice daily for 3 days. Effective and commonly available, but only when local E. coli resistance to TMP-SMX is below 20 percent. Avoid in sulfa-allergic patients.

When Each First-Line Antibiotic Is Preferred
There is no single best antibiotic for UTI — there is a best antibiotic for your situation. Canadian doctors weigh several factors when picking among nitrofurantoin, fosfomycin, and TMP-SMX.
- Choose nitrofurantoin (Macrobid) when: kidney function is normal, you are not allergic to nitrofurans, and the infection is confined to the bladder. It is also generally safe in the second trimester of pregnancy up to roughly 36 weeks.
- Choose fosfomycin (Monurol) when: you have a sulfa allergy, prefer single-dose therapy, have impaired kidney function where nitrofurantoin is contraindicated, or have a history of resistant E. coli.
- Choose TMP-SMX (Bactrim/Septra) when: you have not used it in the last 3 months, you are not in the first trimester of pregnancy or near term, you are not on warfarin or methotrexate, and your local resistance rate is acceptable.
- Consider a urine culture before treatment if: you have had a UTI in the last 3 months, you are pregnant, you are male, or symptoms have not improved on prior empiric therapy.

Second-Line UTI Antibiotics: Cephalosporins and Beyond
When the three first-line agents are unsuitable — usually because of allergy, intolerance, prior resistant culture, or a complicated infection — doctors turn to a second tier. These drugs work, but they are less narrow-spectrum and carry more collateral damage to your gut microbiome.
- Cephalexin (Keflex) — 500mg four times daily for 5-7 days. A common second-line choice in pregnancy and in patients with sulfa allergy. Generally well tolerated.
- Cefixime (Suprax) — 400mg once daily for 5-7 days. Convenient once-daily dosing; useful in selected complicated UTIs.
- Amoxicillin-clavulanate (Clavulin) — 500/125mg three times daily for 5-7 days. Reserved for culture-proven susceptible organisms because empiric resistance is rising.
- Ciprofloxacin or levofloxacin (fluoroquinolones) — now reserved for pyelonephritis or culture-confirmed resistant organisms because of significant side-effect concerns (see next section).

Why Fluoroquinolones (Cipro, Levaquin) Are Now Reserved
For two decades ciprofloxacin was the workhorse of outpatient UTI treatment in Canada. That changed after Health Canada and the FDA issued repeated safety advisories. In 2017 Health Canada updated fluoroquinolone product monographs to warn of disabling and potentially permanent musculoskeletal and nervous-system side effects, including tendon rupture (especially Achilles), peripheral neuropathy, aortic aneurysm, prolonged QT interval, hypoglycemia, and serious mental-health effects such as anxiety, depression, and suicidal thoughts. AMMI Canada now recommends fluoroquinolones be reserved for situations where no alternative exists — primarily pyelonephritis, complicated UTI, prostatitis, and culture-proven resistance to first- and second-line agents. If your doctor prescribes a fluoroquinolone, it is because the benefit outweighs the risk for your specific infection. Patients should be counselled on warning signs (sudden tendon pain, new numbness or tingling, mood changes, palpitations) and contact their doctor immediately if these develop. Older adults, patients on corticosteroids, and those with prior tendon disease are at highest risk.

Antibiotic Resistance: Why Canadian Patterns Matter
An antibiotic only works if your bacteria are still susceptible to it. Public Health Ontario, Alberta Precision Laboratories, BCCDC, and the Canadian Antimicrobial Resistance Surveillance System (CARSS) publish provincial antibiograms — local maps of which drugs still kill which bugs. Three patterns matter for outpatient UTI care across Canada in 2026.
- TMP-SMX resistance — exceeds 20 percent in several provinces, which is the threshold above which guidelines advise against empiric use. This is why your doctor may avoid Bactrim if your culture history shows prior resistance.
- Nitrofurantoin resistance — remains low (typically under 5 percent) for E. coli across Canada, which is why Macrobid has become the preferred first-line agent in most provinces.
- Fluoroquinolone resistance — has climbed steadily over the past decade, reinforcing the move to reserve these drugs.
- Extended-spectrum beta-lactamase (ESBL) producing E. coli — once rare in community UTIs, now increasingly seen, particularly in patients with recent travel, hospitalization, or repeated antibiotic exposure. ESBL strains often require fosfomycin, nitrofurantoin, or intravenous therapy.

UTI Antibiotics in Pregnancy: What Is Safe
Pregnancy changes the calculus. UTIs in pregnancy — including asymptomatic bacteriuria — must be treated to prevent pyelonephritis, preterm labour, and low birth weight. But several common antibiotics are off-limits in specific trimesters. The safest options are typically discussed and confirmed with your maternity provider.
- Cephalexin (Keflex) — generally considered safe throughout pregnancy and is a common first choice.
- Nitrofurantoin (Macrobid) — generally acceptable in the second trimester, but typically avoided in the first trimester due to limited safety data and avoided after roughly 36 weeks because of theoretical risk of neonatal hemolytic anemia.
- TMP-SMX (Bactrim) — avoided in the first trimester (folate antagonist, neural-tube risk) and near term (kernicterus risk in newborn).
- Fluoroquinolones (Cipro, Levaquin) — avoided in pregnancy and breastfeeding due to cartilage and tendon concerns in the developing fetus.
- Fosfomycin (Monurol) — single-dose option that is generally considered acceptable in pregnancy when first-line options are unsuitable.
Complicated vs. Uncomplicated UTI: The Distinction That Drives Treatment
An uncomplicated UTI is a bladder infection in an otherwise healthy, non-pregnant adult woman with a normal urinary tract. A complicated UTI is anything else, and complicated UTIs typically need a longer antibiotic course (often 7-14 days), a urine culture before treatment, and sometimes imaging.
- Men with UTI — almost always considered complicated; rule out prostate involvement and structural problems. Treatment usually 7-14 days.
- Pregnancy — always treated, often with culture confirmation and follow-up culture to confirm cure.
- Pyelonephritis (kidney infection) — fever, flank pain, nausea, vomiting; longer course of oral antibiotics or initial IV therapy.
- Diabetes, immunosuppression, or chronic kidney disease — higher risk of complications and resistant organisms.
- Indwelling catheters, recent urological procedures, or known anatomical abnormalities — culture-guided therapy and longer treatment.
- Recurrent or relapsing infection within 2 weeks of finishing antibiotics — suggests treatment failure or resistant organism.
When IV Antibiotics Are Required
Most UTIs respond to oral antibiotics taken at home. Intravenous (IV) therapy in a hospital becomes necessary when the infection has spread beyond the bladder, when the patient cannot keep oral medication down, or when sepsis is a concern. IV antibiotics commonly used in Canadian emergency departments and hospitals for severe UTI include ceftriaxone, piperacillin-tazobactam, gentamicin, and (for ESBL or carbapenem-resistant organisms) ertapenem or meropenem. Once the patient is stable and afebrile and oral intake is possible, treatment is usually stepped down to an oral antibiotic guided by the culture result. Conditions that typically warrant IV antibiotics include pyelonephritis with high fever or hemodynamic instability, suspected urosepsis, intractable vomiting, pregnancy with pyelonephritis, and immunocompromised patients with febrile UTI. These situations require an in-person emergency department evaluation rather than virtual care.
UTI Not Getting Better — What to Do
Most uncomplicated UTIs improve dramatically within 24-48 hours of starting an effective antibiotic. If you are 48-72 hours into treatment and symptoms have not eased, do not just wait it out. Several things can be going wrong, and each has a different next step.
- Resistant organism — the empiric antibiotic does not support your specific bacteria. A urine culture with sensitivities will identify what will work.
- Wrong diagnosis — interstitial cystitis, overactive bladder, vaginitis, sexually transmitted infection, or kidney stones can mimic UTI. A re-assessment is needed.
- Pyelonephritis developing — new fever, flank pain, nausea, or vomiting means the infection has reached the kidneys and you need urgent in-person care.
- Inadequate antibiotic concentration — for example, nitrofurantoin in a patient whose kidney function does not allow it to reach therapeutic bladder levels.
- Adherence or absorption issue — missed doses, vomiting after the dose, or interactions with antacids or supplements can blunt the antibiotic effect.
Recurrent UTI Prevention: What the Evidence Supports in 2026
Recurrent UTI is defined as two or more infections in six months or three or more in twelve months. Prevention is built in layers, starting with the lowest-risk options and escalating only if needed. Discuss any new supplement or prophylactic antibiotic with your doctor — interactions and contraindications matter.
- Hydration and post-coital voiding — simple, available, and supported by observational evidence.
- D-mannose — a sugar that prevents E. coli adhesion. Several randomized trials suggest a modest preventive effect, with a strong safety profile. Typical dose 2g daily.
- Cranberry products — proanthocyanidin-standardized cranberry extracts have moderate evidence for prevention; cranberry juice itself is less reliable due to variable concentration.
- Vaginal estrogen — for postmenopausal women, topical vaginal estrogen restores the urogenital microbiome and significantly reduces recurrence; available through prescription as creams, tablets, or rings.
- Methenamine hippurate — a urinary antiseptic that converts to formaldehyde in acidic urine. The 2022 ALTAR trial showed it was non-inferior to daily prophylactic antibiotics for recurrent UTI prevention.
- Prophylactic antibiotics — daily low-dose nitrofurantoin or TMP-SMX, or post-coital single-dose prophylaxis, are options for women with frequent recurrences after non-antibiotic strategies have been tried.
The TelePlus Care Virtual UTI Consultation Process
Many uncomplicated UTIs in non-pregnant adult women can be assessed and treated through a virtual visit. Here is what to expect when you book with TelePlus Care. Your visit is reviewed by a licensed doctor, and treatment is provided only when clinically appropriate.
- Step 1 — Intake: complete a secure symptom questionnaire covering onset, severity, prior UTIs, allergies, current medications, pregnancy status, and red-flag features.
- Step 2 — Physician assessment: a licensed doctor reviews your intake and connects with you by video or phone for a 15-20 minute consultation.
- Step 3 — Assessment: many uncomplicated UTIs can be assessed clinically. If a urine culture is needed (recent UTI, prior resistance, treatment failure, pregnancy, male patient), the doctor can provide instructions for local lab testing when available.
- Step 4 — Prescription: the doctor issues an antibiotic prescription, which you fill at any Canadian pharmacy of your choice — Shoppers Drug Mart, Rexall, Save-On-Foods, Loblaws, or your local independent.
- Step 5 — Escalation when needed: if red flags or complicated features are identified, the doctor will direct you to an in-person clinic, urgent care, or emergency department rather than treating virtually.
- Step 6 — Follow-up: a message-based check-in 48-72 hours after treatment confirms symptom resolution and addresses any concerns.
Red Flags That Mean Emergency Care, Not Virtual Care
Virtual UTI care is appropriate for the majority of uncomplicated bladder infections. It is not appropriate when systemic illness or complications are suspected. Go to an emergency department or urgent care immediately if you have any of the following.
- Fever above 38.5 C with shaking chills (rigors) — concern for pyelonephritis or bacteremia.
- Severe one-sided flank or mid-back pain — possible kidney infection or kidney stone.
- Persistent vomiting that prevents you from keeping oral fluids or medication down.
- Pregnancy with any UTI symptoms — needs urgent assessment and possibly culture.
- Confusion, lightheadedness, fast heart rate, or low blood pressure — possible urosepsis.
- Symptoms not improving after 48 hours of antibiotics, or rapidly worsening.
- Visible blood clots in urine, or inability to urinate.
Best Antibiotic for a UTI — Fast, Convenient Virtual Care
Connect with a licensed healthcare provider from the comfort of your home. No referral needed — book your virtual appointment today.
Book Your Appointment NowExplore Our TelePlus Services






Teleplus care clinic is not an urgent care clinic. If you have an emergency please call911 or go to the nearest urgent care facility.